SSPE and MMR vaccine
- Is measles a killer disease or is it actually something else that causes children's deaths to be associated "with" measles?
(Health/Disease?)
- Did measles associated mortality decline before measles vaccine introduction?
- What was the pre-sanitation era measles incidence?
- Reducing the uncertainties: the mortality-case ratio versus mortality-birth ratio:?
- Were 100% of children experiencing measles before measles vaccine introduction?
- Do disease reporting systems remain stable in efficiency? Or does the ratio of reports to actual cases change over time?
- Do measles vaccines prevent measles or cause measles?
- Does " visible healing activity" always correctly reflect the intensity of "the invisible force of disease"?
- Is measles caused by measles vaccines more mild or more severe than natural measles?
- Is there proof that measles cases caused by measles vaccines are more severe than natural measles?
- Does the measles vaccination immunize anyone?
- SSPE and MMR vaccine
Introduction or the "Short Story":
Introduction
or
Measles and it's Vaccines, the "Short Story"
Pre-Vaccine Era: (measles)
What the CDC says:
1. There were 450 deaths associated with measles per year immediately prior to the introduction of measles vaccines.
2. There were 450,00 measles "cases" per year in the pre-vaccine era.
3. The Mortality/Case rate was 1 or 2 deaths per thousand cases.
AND
4. It is claimed that the number of cases cited above are actually "reported cases" and the number is "likely low" as "almost everybody" had the measles in those years.
5. It is also claimed that there was a 99 percent reduction of cases following the introduction of measles vaccines.
What the CDC "forgets" to say:
1. There was a 98% decline in deaths associated with measles prior to measles vaccine introduction.2. The CDC's own evidence shows that the percent of children having measles declined prior to measles vaccine introduction.
3. CDC literature shows that the "live virus" * measles vaccine does not prevent measles but instead causes measles.
4. Measles cases caused by the vaccine are not reported.
5. Measles cases caused by measles vaccines only "appear" milder than natural measles because the vaccination causes immune system suppression.
A suppressed immune system can NOT respond strongly or effectively to the body's needs. Vaccine induced cases are actually more severe than natural measles and thus are accompanied by more adverse events than would occur with natural measles.
6. No evidence exists for claiming that measles vaccine reduces cases of measles. Only natural immunity reduces cases.
7. Numbers five and six (6) above are proved by the larger number of neurologically damaged children (autism) that occur in populations receiving MMR vaccine compared to populations not receiving MMR vaccine.
Introductory Explanations:
Virus
Before we dive into our main theme of measles and associated vaccines, a few words are needed about the star (*) after "live virus" in the summary box above. We understand that virus alone can NOT cause disease.
It can be argued that "live pathogenic virus" do not exist. More commonly, main stream explanations of virology hold that "viral particles" are created when cells die and break into 1000 to 10,000 pieces.
Biologists argue whether these cell fragments are living virus or are
simply chemical debris. For our purposes it is important to know that virus are created when cells die or stated plainly,
virus are created by illness — but the illness is not created by the virus. Cells die only when a severe chemical
imbalance exists within the cell. This severe imbalance occurs when the cell is either poisoned or malnourished. The poison may come from outside the body or may be generated by incomplete
digestion within the body. Virus created by diseased cells are essentially inert, meaning dead and chemically inactive. None the less, for the purposes of this web page, a conventional understanding of the "live virus theory"
will lead one to correct conclusions about the harm caused by "live virus" injections if one imagines that a serious challenge to the immune system occurs when
multiple types of "live virus" are injected and the assault is intensified by the far greater assaults of decaying material and poisonous chemical additives present in the vaccine. The standard ingredients of MMR vaccine are: chick embryo
cell culture (decaying), human diploid lung fibroblasts, salt, amino acids, fetal bovine serum,
sucrose, sodium phosphate, glutamate, recombinant human albumin, neomycin, sorbitol and hydrolyzed gelatin.[1]
Health
Some important factors bearing on childhood health are breast feeding by a healthy mother and historically, the reforms which have let to a prevalence of sanitation, year around nutrition and
hygiene. Other principles of natural health play a role as well. Prior to reforms that began around the year 1750,
large cities typically lacked all the
protection conferred by nutrition, sanitation and hygiene. Sanitation today in
the "developed" world is advanced to the point where we can largely take it for granted. Hygiene too is largely a given. However nutrition and other natural health principles are still poorly understood and
incompletely practiced although modern transportation combined with freezers and refrigerators
have helped produce vast improvements in providing a year around availability and wide variety of fresh foods compared with former times.
As a result, life span has increased and serious infectious diseases are little heard of today.
Measles, a safe disease:
This article is about measles and measles vaccines
so information on why minor diseases (a.k.a. acute healing episodes) such
as measles, mumps, rubella and chickenpox are not to be feared and indeed should be regarded as safe and even beneficial milestones in childhood development will be found elsewhere although we are
touching on the subject briefly.
The symptoms of contagious disease are typically fever, rash, mucous, swollen lympth glands and increased urination and defecation. All these symptoms are the visible signs of healing activities, mainly detoxification, that are
typically intense in nature and shorted lived giving rise to the description: acute healing episode. Safe and beneficial are of course appropriate
descriptions for acute healing episodes only if quality
nutrition is understood and present in the child's diet. Also proper care during illness must be understood and practiced. There are three common reasons why children suffer adverse side effects of acute diseases and these
basically resolve to malnutrition, improper treatment of the illness and serious underlying diseases other than the minor acute infections of measles, mumps, rubella or chickenpox.
Children do not die from measles and when death occurs with measles, one or more of the three true causes of
death were present. Children who suffer with severe cases of measles, typically, are deficient in vitamin A and vitamin C.[2] Children with measles are also typically medically mistreated by suppression of their fevers.
Fever is a natural mechanism which restores health and thus fevers should not
routinely be suppressed. Also, children should not be forced to eat when not hungry, especially at a time when the body needs to direct its energy into healing rather than digestion.
When a child dies with measles in
developing countries it is likely than nutrition was the key missing element. In developed countries, the key is usually that there coexisted a much more serious
underlying disease condition such as cancer although a deficiency of vitamins A and C often play a role. For more information about natural health and treatment of acute diseases see: [3]
The CDC has posted on their web pages that in the years immediately before the measles vaccine introduction there were:
It is often stated that the CDC's case number is actually 'reported cases' and it is believed the true number of yearly cases were higher. Some other pro-vaccine web sites claim nearly 100 percent of the children born had measles in the pre-vaccines era and cite numbers such as three or three and one-half million cases. There have been "news" announcements that measles is no longer endemic in the Americas. (2000 USA, 2002 the Americas)
There are several problems with the official statements above.
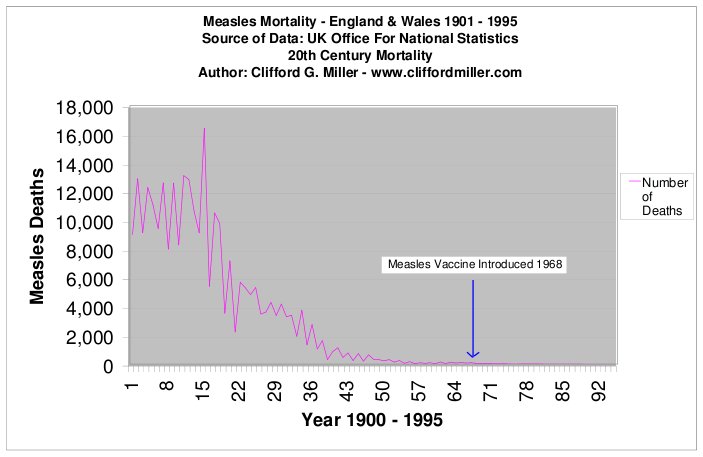
Measles associated deaths declined 98% before vaccination: The number of children dying of measles went down by 98% or more before the introduction of the vaccine. This is undisputed. Why is this fact seldom or never mentioned in the popular press?
It is certainly a relevant fact when one is making an informed decision. While all or almost all children likely did have measles in the pre-sanitation era, the 98% decline in deaths prior to vaccination
brings into question the allegation that "everybody"
had measles immediately prior to measles vaccine introduction. For measles, the pre-sanitation era is not the same as the pre-vaccine era. The pre-vaccine era for measles is the period immediately prior to the vaccine introduction.
Sanitary improvements with accompanying nutritional improvements made a slow but
radical transformation of living standards over two centuries of time by greatly reducing malnutrition and reducing filth in water and air especially in the larger cities. [more]
The number of children dying of measles went down by 98% or more before the introduction of the vaccine. This is undisputed. Why is this fact seldom or never mentioned in the popular press?
It is certainly a relevant fact when one is making an informed decision. While all or almost all children likely did have measles in the pre-sanitation era, the 98% decline in deaths prior to vaccination
brings into question the allegation that "everybody"
had measles immediately prior to measles vaccine introduction. For measles, the pre-sanitation era is not the same as the pre-vaccine era. The pre-vaccine era for measles is the period immediately prior to the vaccine introduction.
Sanitary improvements with accompanying nutritional improvements made a slow but
radical transformation of living standards over two centuries of time by greatly reducing malnutrition and reducing filth in water and air especially in the larger cities. [more]Measles incidence in the pre-sanitation era:
In the 1800's and early 1900's it is likely that nearly every child had measles. This period should be considered as the pre-sanitation era although considerable nutritional changes were also occurring and the combination of changes lowered measles mortality greatly prior to the pre-vaccine era. However, it is rather cumbersome to call a period of time the pre-effective-sanitation-and-nutrition-era. It is misleading to name the pre-sanitation era as the pre-vaccine era.The pre-vaccine era is the years immediately prior to 1963 when the first measles vaccine was introduced. Mortality associated with measles was approximately one death in 200-250 cases in the pre-sanitation era. Due to improved nutrition and sanitation, this mortality ratio fell greatly but because we are given uncertain figures about measles incidence in the pre-vaccine era, there is equal uncertainity in calculating the degree that the mortality-case ratio fell.
Even worse, is failing to understand the formula which locks mortality and cases together. For a fixed number of deaths, for example 450, the mortality-case ratio can be large (1 or 2 per 1000 cases) only if the number of cases are low, in this example 225,000 to 450,000 cases. If on the other hand, for 450 deaths and a mortality-case ratio of 1 per 10,000 cases, then the number of cases is 4.5 million. A misleading presentation of the facts can lead some lay persons to believe that there was 1 death per 1000 cases and everybody had measles, thus approximately 4 million cases. That scenario would be impossible unless the number of deaths were 4,000.
Mortality-case ratio versus mortality-birth ratio:
If we accept the CDC's figure of 450 deaths per year associated with measles and
about 4.2 million live births per year, then
for approximately every 9300 children born, one would die with measles. Official literature confirms this approximate figure and even states that in industrial countries "the measles fatality rate is 1 per 10,000 cases..."[4]
It is possible and likely closer to reality to consider the mortality-case ratio was one death per 1000 cases but only one child in 10 had measles, an equivalent way of looking at the "1 per 10,000" mentioned above.
The CDC maintains that in the vaccine era (1985) the case
mortality was .2% (.002) which is another way of saying 1 in 500. Low mortality-case ratios (1 or 2 deaths per 1000 cases) support our contention that measles incidence declined before the introduction of measles vaccines.
Measles incidence in the pre-vaccine era versus the pre-sanitation era:
 There are at least five reasons why we know that measles incidence declined prior to the introduction of the measles vaccine:
There are at least five reasons why we know that measles incidence declined prior to the introduction of the measles vaccine:
- The 98% decline in mortality associated with measles.
- The CDC's reported cases do not take into account the increased population of children in 1960's versus the 1920's.
- The 50% measles incidence following the first "live virus" measles vaccine.
- The tendency of the error prone reporting system to auto-compensate for long term changes.
- The fact that CDC statistics fit without adjustments. These facts are discussed below
According to the CDC, reported cases in the 1920's were only slightly higher than reported cases (probably "adjusted" reported cases) immediately prior to the measles vaccine introduction in 1963. However, the population of children was considerably higher in 1960 than in 1920 which means there was a decline in the percentage of children experiencing measles.[more]
The first "live measles vaccine" caused one-third of the recipients to develop
a high fever and half of the recipients to develop
a rash.[more] There can be no stronger exposure to measles than a direct injection of decaying material, toxic chemicals and "live virus." The proof that vaccine induced measles is more severe than natural measles is shown by the
higher percentage of children suffering from vaccine injury than
occurred as side effects of natural measles. Thus the number of measles cases following direct injection of vaccine ingredients can easily be higher than would occur following multiple natural measles exposures.
The number (50%) of vaccine recipients with rash following
the first "live virus" vaccine suggests that natural immunity to measles must have been a minimum of 50% of the children at that time and given the force of disease when toxic ingredients are directly injected,
natural immunity was likely to have been considerably higher than only 50%. The 200,000 to 600,000 reported cases of measles each year may be reasonably accurate in the pre-vaccine era as simply cases and require
no further adjustment for accuracy.
Denying that measles incidence declined prior to vaccine introduction is thus contrary to data obtained from the first "live virus" experiments and ignores the fact that reported cases (or "adjusted" reported cases)
remained nearly the same in spite of increasing childhood population and is not sustainable due to uncertainties in the reporting system which we discuss below.
Conclusion: Measles incidence in the pre-vaccine era had declined from the pre-sanitation era by at least 50% (as a percentage of children over age one) and as much as 90% before measles vaccination began.
When did measles incidence began to decline?
It appears that the decline in the percentage of children having
measles may have begun much earlier than generally thought as revealed by a study of measles epidemics performed on the years 1900 to 1931 that led a researcher named Hedrich to observe
epidemics of measles only occurred when less than 68% of children had
developed a natural immunity to measles. This observation lead to the theory of herd immunity. [more] Hedrich's observations of the natural cycle of measles may have been unrelated to his theorized herd immunity as herd
immunity has never been proven.
A large number of measles cases occurred each year in the study period yet most children had measles only
once before age 15. This suggests that many children were exposed to measles several times before exhibiting signs of classical measles. Individual immunity is not an unchanging value, but
changes day to day and only when the amount of toxins in an individual's body builds beyond a critical point will the child's body require an acute detoxification that is carried out by fever, rash, mucous, etc.
Without this high level of toxins to
constitute "susceptibility" multiple exposures to so called "pathogenic virus" would occur without symptoms. It is possible that less than 100%
of children were experiencing measles in the 1920's and possibly even earlier. If measles case reports in the 1920's already represented less than 100% of the theoretical susceptible population, then a bias is created that
means we over estimate measles incidence not only for the 1920's but also for the 1960's.
Do reporting systems remain stable in percent of cases reported?
Reporting systems can under-report as well as over-report. In the 1920's approximately 19 percent of cases were reported based on the concept that 100% experienced measles.
By the time the measles vaccine was introduced, it is possible that "reports" were
adjusted upward by state health departments before the state "adjusted reports" figures were relayed to the CDC. This problem is illustrated in Dispelling Vaccination Myths by Alan Phillips, part 3,
"In 1974, the CDC determined that there were 36 cases of measles in Georgia, while the Georgia State Surveillance System reported 660 cases."
(credited to Keith Block, M.D., a family physician from Evanston, Illinois)[5]
 This problem of case reports versus actual cases is further illustrated by case reports in recent years.
Vaccine-induced measles symptoms occur consistently year after year, yet the CDC states there were 44 reports of measles in 2002 and only 37 reports in 2004.
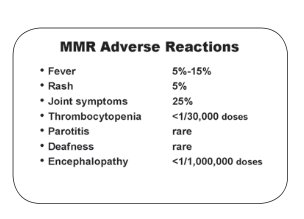
Yet official CDC figures admit that for the MMR vaccine:
This problem of case reports versus actual cases is further illustrated by case reports in recent years.
Vaccine-induced measles symptoms occur consistently year after year, yet the CDC states there were 44 reports of measles in 2002 and only 37 reports in 2004.
Yet official CDC figures admit that for the MMR vaccine:
Do "live virus" vaccines "prevent" disease?
Given that it is acknowledged that the MMR vaccine is followed with a measles-like rash in 2.1% (84,000) of the children within 5 to 15 days and nearly 15% have fever, it follows that even if one credits all the reported cases of natural measles (only 58 reported cases in a recent year) to the unvaccinated, and then multiplies the reported number by 5, (5 x 58 = 290) the case to report ratio of the 1920's, then unvaccinated children have less than a one percent attack rate or alternately stated have in excess of 99% immunity while only 95% immunity is claimed for the vaccinated.
Thus we need to combine three ideas, first, that a natural decline in measles incidence occur ed before the introduction of the measles vaccines and this
natural decline continued to occur in the unvaccinated after the introduction of vaccinations.
Secondly, that 600,000 cases of "measles" fever and 200,000 rashes that occur in the two weeks following MMR vaccination are actual cases of vaccine induced measles.
And thirdly, that unvaccinated children have low rates of measles incidence, on the order of 1 or 2 percent if we can believe that the CDC measles reporting system is meaningful for
cases outside of the 600,000 cases caused by the MMR vaccine.
In the light of the few acknowledged measles reports, it becomes obvious that the measles vaccine,
a so called "live virus" vaccine, does not prevent measles but rather causes measles. Actually, this fact is admitted in the official Merck and CDC sources as noted above.
According to the measles chapter of the Pink Book, a standard CDC reference,
the measles vaccines does cause measles in susceptible children but the cases are stated to be mild. The pro-vaccine theory is that these "mild" cases are safe and immunize
the child against "severe cases of natural measles."
Are these "mild appearing" cases actually mild in reality?
To understand this question we must know the difference between visible healing forces and invisible disease forces. Simply put, mucous, diarrhea, increased urination, rash and fever are the manifestation of healing force
sometimes termed an immune system response. Normally, the higher the fever or the more rash spots the more severe is the force of the disease. However, if
the immune system is suppressed or compromised, the strength of the visible healing forces will be weak even in the face of severe immune system challenges. In such a case,
the mild appearance of healing force is not an accurate measurement of the intensity of the vaccine ingredient challenge. It is documented that vaccines, including the MMR suppress the immune system. The CDC
recommends that a tuberculin skin test not be given from one day to a month after month after receiving an MMR vaccine due to immune system suppression. Children with a compromised immune system may react with less fever.
It is also documented that measles can occur without a rash in
immunocompromised children.[suppress] Also, in Africa, it was found that children with more severe symptoms of measles had better survival rates than children with milder symptoms.
[7]
Are vaccine induced measles cases more or less mild than natural measles cases?
What measurement would give an accurate indication of the severity of vaccine induced measles disease? It is claimed that the relatively rare cases of Subacute Sclerosing PanEncephalitis (SSPE) and Encephalitis that occurred
following natural measles has all but disappeared following vaccination. Both of these encephalitis diseases are basically an irritation or inflammation of the nervous system and brain. Is measles vaccine rightfully credited with
creating a decline in brain and nerve irritation associated with measles? We must answer an emphatic NO. What was sub-acute, that is beneath obvious intensity, and acute has become super acute and chronic and is therefore called
today - autism and autism spectrum disorders. What affected approximately 1 child in 10,000 in the pre-vaccine era now affects 1 in 150, about a 60 times increase, and recent studies suggest that 1 in 67 is a more accurate number of children affected by some degree of autism
spectrum disorder which basically is a collection of symptoms relating to brain and nerve inhibition or destruction.[more] Our opponents will of course reply that they have 30 good studies and that no connection between vaccines,
especially the non-mercury containing MMR vaccine, and autism can be found. However this is a lie agreed upon by government and industry talking heads. The largest study in the "30 good studies" is the Danish MMR study which showed
that children who received 6 vaccines in the first year of life had 48.6 autistic children per 100,000, while children who received the same 6 vaccines plus the MMR at 15 months of age had 61 cases of autism per 100,000. This is
a clear indication that MMR makes a significant contribution to causing autism. The study population size, 535,303, is quite adequate for drawing accurate conclusions. In a supporting vein, the second largest study in the Yokohama
Prefeture in Japan found that when the MMR vaccine was with drawn from the market that the rate of autism fell in the population not receiving MMR. When the triple antigen MMR vaccine was replaced with 3 separate vaccines
given close together in time, then the rate of autism resumed its upward climb.[8]
Therefore, MMR and other measles vaccines contribute to the increased rate of autism spectrum disorders (nerve and brain damage) as compared to unvaccinated children. Vaccine induced measles cases are severe rather than mild. These severe cases are caused simultaneously with significant immune system suppression so children only appear to have "mild" disease as evidenced by lower fever, shorter time of fever and frequently no rash. What is observed is not the hidden forces of disease but rather the visible working of the body's healing mechanisms. Following vaccination the obvious working of healing power is weak and inefficient and the disease is not fully healed and residual nerve and brain inflammation occurs at a higher than with natural measles.
Are the vaccinated who come down with a case of severe measles immunized?
This question is basically answered above where we show that the measles vaccine causes measles and does not prevent measles. A better understanding occurs when it is known that the
antibody theory is does not predict immunity. Individuals with low or zero antibody count are as likely to be immune as individuals with medium to high antibody count.
Very high antibody counts are likely to correspond to an active immune response indicating
disease rather than indicating immunity. [9] A better predictor of immunity is the level of toxic ingredients in the body. The higher the toxic level becomes either normally or by an injection, the more likely the body will need to detoxify
using acute mechanisms of fever and rash to
accomplish a return to normal which is the true state of immunity. Immunity is a result of health and not a result of either disease or vaccination.
Worse, when ingredients are directly injected into a body the full detoxification necessary for a return, to natural immunity occurs slowly and typically remains incomplete for years. If the immune system is
suppressed as is typically the case with vaccinations, a full detox is impossible and the child is left as susceptible or even more susceptible than before the vaccination.
However, the immune suppression caused by the MMR vaccine as well as other vaccines typically given simultaneously with MMR means the numerous injected ingredients are
harder to remove than naturally acquired toxicity and the child's body may take years to establish a normal immunity, if ever.
Vaccinated children only partially detoxify, that is some of the toxic ingredients remain in the body. This means that vaccinated children are more susceptible to further cases of measles and other infectious diseases. The 95% estimate of immunity for vaccinated children may be high. Left unvaccinated, the bodies of most children will remove any naturally occurring toxic compounds and thus any cellular imbalances are removed that are the true cause of susceptibility which is but a need to detoxify. In unvaccinated children, this removal usually occurs naturally without symptoms of rash and fever. When there is fever or rash or both in well nourished children, the process is safe and produces a full return to immunity provided the child is not subject to the common forms of medical mistreatment. In fact, such natural disease is considered by some to be a developmental milestone because there will be a spurt of growth, physically, emotionally and mentally. Often childhood ailments such as asthma and allergies are left behind following the healing of measles and similar diseases. .
Adolescent children commonly acquire more toxicity as shown by teenagers tendency to develop pimples and boils. Previously vaccinated teenagers are subject to a higher rate of severe measles than are unvaccinated children.
This occurrence of severe measles in teenage years is not because a non-existent vaccine immunity wears off. Rather,
the additional acquired toxicity that occurs in adolescent years adds to the residual vaccination toxicity and the body arrives at a point where an acute detoxification is necessary. Therefore vaccinated children have less
real immunity to measles than do children that have had natural measles. This is admitted. In our opinion, vaccinated children do not have as great as immunity to measles as children who are never vaccinated and
who never contract measles because of their naturally occurring immune state. Real immunity is based on a clean blood stream that is well nourished. Or as we often say, "health is the only immunity."
Conclusions to the "short story":
The statements above will seem radical to many individuals. In our reference section below are appended various charts, information and links to information to help you with your journey of discovery.
and expanded reference section.
and 90 % had the disease by the time they were 15. (CDC history and Pink Book)
and 3% more cases occur in the over 15 year old population (Neil Z Miller)
Measles Statistics:
1920-1929: 467,000 reported cases average per year with 2.4 million children added to susceptible group each year.
1959-1962: 440,000 reported cases average per year with 3.9 million children added to susceptible group each year.
[Colonial Times to 1970 Census info]
According to a CDC Measles Data Page, following are the deaths associated with measles from 1950 to 1966
Year: 1950 1951 1952 1953 1954 1955 1956 1957 1958 1959 1960 1961 1962 1963 1964 1965 1966 Deaths: 468 683 618 462 518 345 530 389 552 385 380 434 408 364 421 296 261
What decline in deaths associated with measles
occurred before measles vaccination?
Measles associated deaths - USA (CDC)
1900-1909: 8377 deaths per year (average) associated with measles.
1920-1929: 6659 deaths per year (average) associated with measles.
1953-1962: 444 deaths per year (average) associated with measles. (CDC states 450/yr)
1959-1962: 404 deaths per year (average) associated with measles.
In 1920-1929, the average number of deaths were 6659 in a population where 2.4 million children susceptible to measles were added each year.
The 2.4 million measles susceptible children added each year in the 1920's is less than the average of 2.9 million babies born per year. First, because there was very high mortality in the first year of life and almost no measles cases occurred in the first year of life. Only about 1 percent of cases occurred between the first and second birthdays. Secondly, because the population was rapidly increasing, the average population per year for children in the 5-15 year old range was also lower than the average number of children per year in the 1 to 5 year old group. This average number of children per year in these age groups lowers the estimate of theoretical susceptible population. [Source of data: Census figures, Colonial Times to 1970]
A 96 percent drop in death rate associated with measles occurred in only 40 years, in the USA. (1920-1960) If we begin in 1900, the decline in death rate over a sixty year span from 1900-1960 was about 98%.
Death per Cases Versus Death per Births Using the average of 8377 deaths per year, 1900-1909, and 2 million susceptible children (rough estimate), then one child died for every 238 cases of measles or one death per each 272 births. These are rough estimates. From 1953-1962, using the CDC figure of 450 measles death per year at a time when there were an average of 4.1 million births per year gives measles death to birth ratio of 1 in 9,111 children. From 1959-1962, 402 children per year died of measles with about 4.2 million added to the susceptible group per year giving one child dying of measles for each 10,448 born.
Formulas: change one number and other numbers must change as well:
Some vaccine proponents would like us to believe that almost everybody had measles before the measles vaccine was introduced and thus the number of "reported" cases of 450,000 represents about 3.6 to 4 million actual cases.
At the same time, the report of 1 death per 1000 cases is something some people seem to believe is fixed. However, the deaths, cases and the death/case ratio are numbers locked together in the formula:
Death/Case-Ratio = number of deaths divided by number of cases.
likewise deaths times the inverse of case/death-ratio = cases. Examples: 450 deaths per year with various death/case ratios:
450 deaths times 1000 (1 death per 1000 cases) = 450,000 cases (not reports
450 deaths times 500 (1 death per 500 cases) = 225,000 cases
450 deaths times 9000 (1 deaths per 9,000 cases) = 4,050,000 cases
450 deaths times 10,000 (1 deaths per 10,000 cases) = 4,500,000 cases.
It should be noted that that from 1954 to 1964 more than 4 million babies were born each year with a peak of 4.3 million born in 1957.
The CDC is an official source of statistics. Unfortunately, one branch of the CDC receives 2.1 billion dollars per year to promote vaccines. People hired by the CDC are believers in the power of vaccines to prevent disease and of a belief system that promotes "vaccinations are immunizations" paradigm.
.
It is hard to have confidence in figures that the CDC obviously does not themselves believe. That is the 450,000 measles cases are also labeled as reports of measles, meaning that the true number of cases are believed by some vaccine proponents to have been much higher, perhaps nearly 100 percent of the birth cohort or over 4 million cases per year in the 1950's. We will show below that a decline in the percentage of children had already started prior to the introduction of measles vaccines. In the controversial arena of epidemiology where estimates must be made, the most reliable figures tend to be death figures, at least before a vaccine is put on the market to cause deaths associated with the disease in vaccinated individuals as well as deaths associated with the vaccine to be attributed to other causes. You can see from the CDC graph below that 450 measles associated deaths per year prior to the introduction of measles vaccines is a "reasonable" number. It can be argued that the true pre-vaccine number was considerable lower 450 per year or even that all deaths attributed to measles are actually due to other causes but we will not go into that phase of this subject here.
Measles deaths - USA (Vital Statistics)
Source: http://www.healthsentinel.com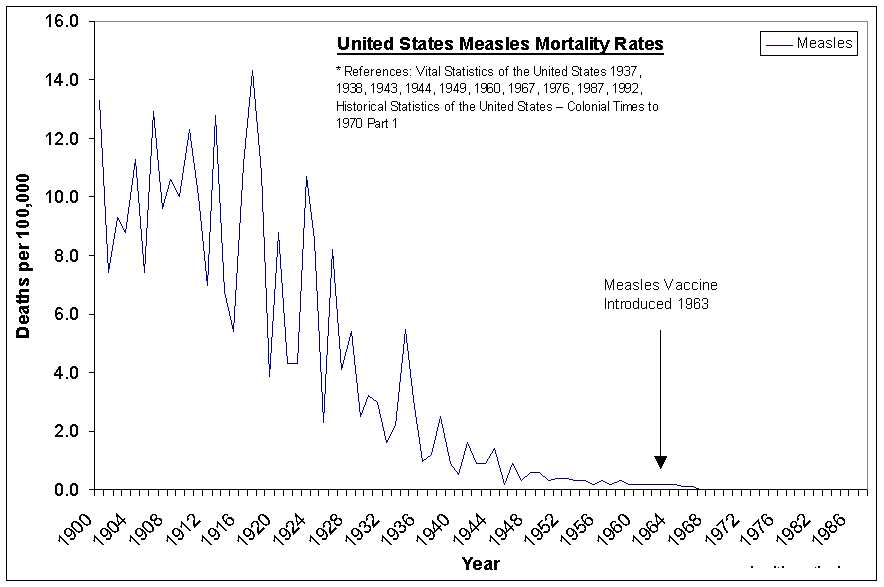
Measles Case/Mortality Ratio versus Birth/Mortality Ratio
A quick glance at the chart immediately above shows that in 1900 through 1924, about 10 deaths per year per 100,000 population would be a fair average.
Measles occurred primarily in children over 2 years of age. Only one percent of cases were in children between 1 and 2 years of age. In 1961 the death rate associated with measles was .237 per 100,000 population. This decline from 10 to .237 per 100,000 population represents about 98 percent decline in mortality that occurred before measles vaccination was started.
In the 1950's, there were births varied from 3.6 to 4.3 million per year with 450 deaths associated with measles per year.
While the following figures are rough, they show a vast change in death rate:
Near 1900: For 2,000,000 Children (births/year) divided by 10,000 deaths = one measles associated death per 200 births or more appropriately, due to high infant mortality due to other causes, one measles associated death for every 238 measles cases.
In 1950's: For 4,300,000 Children (births/year) divided by 450 deaths = one child's death was associated with measles for every 9,556 births.
Stating the conclusion by "deaths per number of births" (Birth/Mortality Ratio), makes it clear that there was a tremendous drop in deaths associated with measles. This method also avoids controversial questions about how many cases of measles occurred each year and thereby the question of what the Case/Mortality ratio was prior to introduction of the vaccine. Of course, we can only side step those questions temporarily and will address them below.
But first some more statistics in a graph showing the decline in deaths from measles in some other countries:
Conclusion 1. It is a fact that Birth/Mortality ratio for measles deaths dropped by 98% or more before the introduction of measles vaccines. This conclusion is not controversial.
What about the CDC claims for Case/Mortality ratio?
(Pre-vaccine era: 450,000 cases, 450 deaths, 1 death per 1000 cases)1. CDC figures above "fit" without adjustment.
2. Post-vaccine, CDC states Case/Mortality rate in 1985 was 1 death per 500 cases.
3. CDC states Case/Mortality rate in 1950's was 1 or 2 per 1000 cases.
(2 deaths per 1000 cases = 1 death per 500 cases.)
So what is going on as far as the number of real measles case incidence is concerned?
What decline in measles incidence
occurred before measles vaccination?
Lets review: 450 deaths, 1 or 2 deaths per 1000 cases and 450,000 cases in 4 million children born per year. (approximate)
For sake of argument, we agree to use the 450 deaths as a starting point although numbers less than 100 could be argued.
The numbers above are locked together: 450 deaths at 2 deaths per thousand cases means 450 times 500 = 225,000 cases 450 deaths at 1 death per thousand cases means 450 times 1000 = 450,000 cases 450 deaths at 1 death per 9,556 cases means 450 times 9,556 = 4.3 million cases. So what is the problem? Simply put, if we doubt the case number is correct, then we must change the Case/Mortality number.
If the cases were near 100 % of the child population, then the Case/Mortality Ratio must be changed to 1 in 9556. Yet, the CDC maintains that in vaccine era (1985) the case mortality was .2% (.002) which is another way of saying 1 in 500. The real question here is which of the following three scenarios are correct:
We have to wonder, does the CDC actually know the Case/Mortality ratio? Or is the real problem a belief system that simply can not believe that measles incidence declined in the pre-vaccine era? If measles declined as a result of factors other than vaccines then measles vaccines are seen as less important or even as worthless.
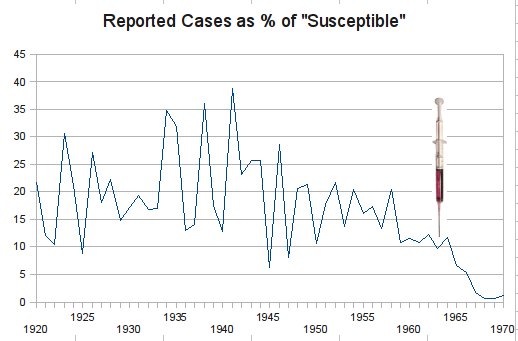
Reported cases were about the same number in the 1920's as in the early 1960's
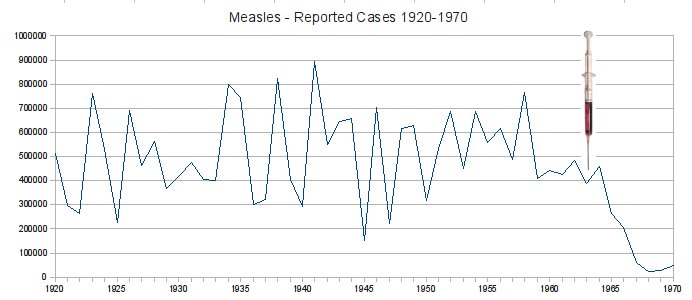
Notice the reported cases from 1959 to 1962, are about 440 to 450 thousand average case reports per year just as the CDC says. While it might not be obvious, the reported cases from 1920 through 1929 average 467 thousand cases per year. So what does nearly the same or slight decline in reports in these two time periods really mean?
Child population in 1920's much less than in early 1960's
In the 1920's, about 2.4 million children were added to the measles susceptible population each year. In the 1960's, about 3.8 or 3.9 million children were added to a theoretical measles susceptible population. Did the reporting system change in effectiveness, or did cases decline, or both?
The 467 thousand reported cases in 1920-1929 represents a high percentage of the children susceptible to measles each year, perhaps nearly 100% incidence, The baseline for the same percentage of childhood measles incidence in 1959-62 would have been 726 thousand reported cases due to the increased childhood population. Because only 440 thousand cases were reported, this constitutes approximately a 39 percent decline in cases and as stated elsewhere, the true decline is likely to be a minimum of 50% and as much as 90% by 1963, the year that the first two measles vaccines were introduced. This is easier to see in our next graph which shows the reported cases plotted against the dramatically rising population.
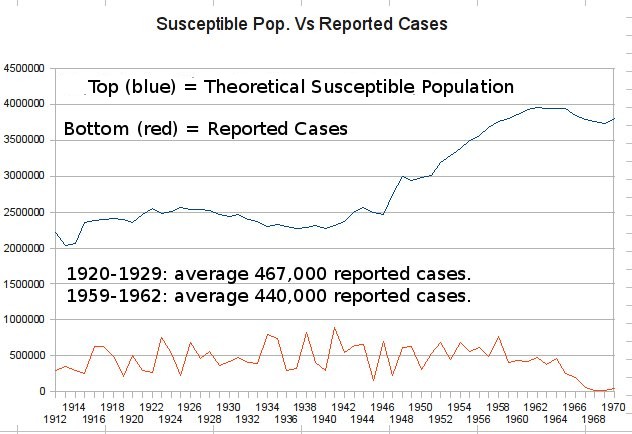
Above: Measles cases reported as a percentage of the theoretical susceptible population.
Source of graph below: http://www.phac-aspc.gc.ca/publicat/pch/vol3supb/figures/fg7_e.gif
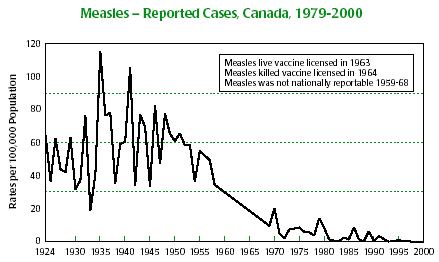
The graph above shows measles cases per 100,000 population in Canada had begun a decline before measles vaccine was introduced. A less clear version of the Reported cases in Canada is available at: ije.oxfordjournals.org/cgi/reprint/28/1/141.pdf and is shown below.
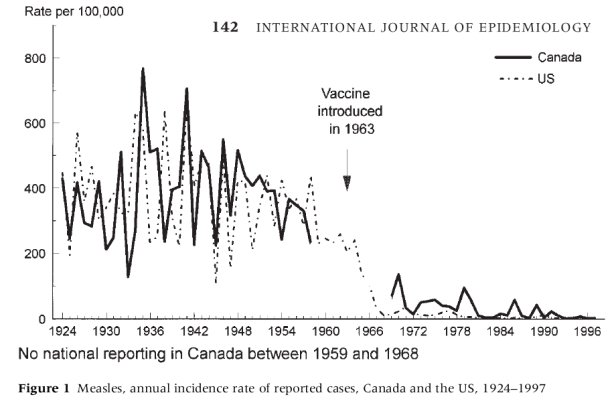
The graph above of combined US and Canada measles figures is credited to the International Journal of Epidemiology 1999;28:141–146 © International Epidemiological Association 1999 Printed in Great Britain.
The percentage of children in our population per 100,000 persons has stayed about the same. The graph above shows that the reporting of measles by 100,000 population in both Canada and the USA went down before the measles vaccine introduction. The above two graphs show the same decline as our own graph for Reported Cases as % of "Susceptible" created from census figures.
Did 100% of children experience measles in the 1920's?
Do you remember when we wrote above,
If the 467 thousand reported cases in 1920-1929 represents a high percentage of the children susceptible to measles each year, perhaps nearly 100% incidence,...?
So when exactly did measles begin declining in incidence? The graphs from the International Journal of Epidemiology suggest the decline began
about 1935 or 1936. Graphing reported cases as a percentage of susceptible children suggests that the peak was 1941 when the USA experienced almost 900,000 reported cases of measles which thereafter declined.
However, the original work on "herd immunity" suggests that measles may occurred in less than 100% of children even earlier.
http://www.vaccineriskawareness.com/The-Herd-Immunity-Theory-Treating-Our-Children-Like-Cattle
"The herd immunity theory was originally coined in 1933 by a researcher called Hedrich. He had been studying measles patterns in the US between 1900-1931 (years before any vaccine was ever invented for measles) and he observed that epidemics of the illness only occurred when less than 68% of children had developed a natural immunity to it."How did less than 68% of children develop "immunity" if 100% of the children had the measles?
It is not only death rates that decline with advancing sanitation and nutrition but also the incidence of disease. An example of natural immunity to measles can be seen in a medical article that revealed that the unvaccinated Amish in Lebanon County, PA had no measles cases from 1970 though December 1987. This group was large and yet had no cases for 17 years while mainstream medicine was crediting low measles rates to vaccination. Measles among the Amish: A comparative Study of Measles Severity in Primary and Secondary Cases in Households Published by The Journal of Infectious Diseases 1991:163:12-16, page 12.
Another source, Adverse Events Associated with Childhood Vaccines: Evidence Bearing on Causality http://books.nap.edu/openbook.php?record_id=2138&page=118, OCR for page 119:
Development of a live attenuated measles vaccineIf a "live virus" plus toxic vaccine ingredients directly injected into a child can cause only 50% of the children to become ill, then natural immunity must have been at a minimum of 50% and could easily have been higher because there is no stronger "exposure" to a disease's cause than direct injection of toxic compounds. We will prove later in this web page that vaccine caused cases are severe not "mild".
... The initial vaccine was derived from the Edmonston strain, which was attenuated by serial passage in various tissue cultures and ultimately grown in chicken embryo cells. The resulting variant was named the Edmonston B strain. It was quite immunogenic, but it was not free of side effects. One-third of the recipients developed high fever, and half of the recipients had a rash. Nevertheless, none of the recipients acted ill.
As we mentioned earlier, reporting systems can under-report as well as over-report. In the 1920's approximately 19 percent of cases were reported. By the time the measles vaccine was introduced, it is possible that "reports" were adjusted before relaying to the CDC and thus could have possibly represented an over reporting of the true number of cases. This problem is illustrated by Dispelling Vaccination Myths by Alan Phillips, part 3,
"In 1974, the CDC determined that there were 36 cases of measles in Georgia, while the Georgia State Surveillance System reported 660 cases."
(credited to Keith Block, M.D., a family physician from Evanston, Illinois)[5]
This problem of case reports versus actual cases is further illustrated by case reports in a recent year, merely 58 measles cases were reported. Why were the measles cases which follow within two weeks of the measles vaccination not reported? In earlier years, according to the University of Maryland Medical Center, "About 5% to 15% of people who are vaccinated with any live measles virus vaccine develop a fever of 103 degrees or greater, usually between five and 15 days after the vaccination." Surely natural immunity was not less than 85% to 95% in 1971 when MMR was licensed. Tests which used MMR and chickenpox vaccine as a control for the combination of four vaccines, MMRV, preformed after 2000 showed 14.9 percent of recipients experienced fever in the two weeks after vaccination.
Following vaccination with a "live virus",
Do all susceptible children get the disease?
Adverse Reactions Following Vaccination
The following is a quote from the CDC's measles chapter of the "Pink Book":The measles chapter of the "pink book" can be found on the CDC website at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf
Fever is the most common adverse reaction following MMR vaccination. Although measles, rubella, and mumps vaccines may cause fever after vaccination, the measles component of MMR vaccine is most often associated with this adverse reaction. After MMR vaccination, 5%–15% of susceptible persons develop a temperature of 103 F (39.4 C) or higher, usually occurring 7–12 days after vaccination and generally lasting 1–2 days. Most persons with fever are otherwise asymptomatic.
Measles- and rubella-containing vaccines, including MMR, may cause a transient rash. Rashes, usually appearing 7–10 days after MMR or measles vaccination, have been reported in approximately 5% of vaccinees.
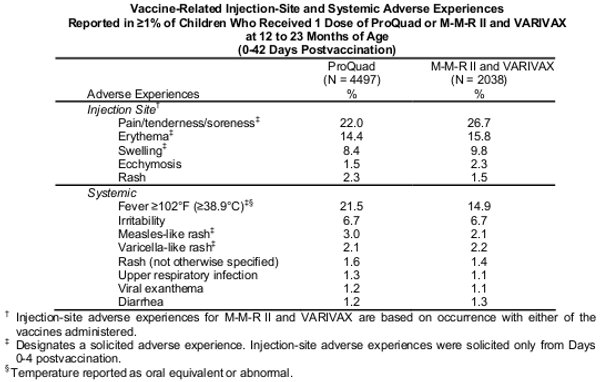
In more recent trials of the MMRV (Measles, Mumps, Rubella and Varicella/Chickenpox) using the MMR and a varicella vaccines as controls, you can see below that 14.9 percent of recipients of MMR still have fever equal to or greater than 102 degrees and 5.7 % had a rash of which 2.1% were measles-like, 2.2% were varicella-like and other rash 1.4%. If 4 million children were vaccinated that would mean 84,000 with measles like rash and 56,000 with undefined rash. For fever, the total rises to 14.9%, a whopping 596,000. So why are these 84,000 minimum and near 600,000 maximum number of measles cases not reported? These numbers are only for the first vaccination between 12 and 23 months of age.
Conclusions: Natural Immunity
A natural decline in measles started prior to measles vaccination.
1. Reported cases as a percentage of susceptible population declined prior to vaccination.
2. Early "live virus" vaccine trials showed natural immunity to be 50% or more.
Some CDC officials mistrust their own reporting systems.
1. Chickenpox reports declined. The CDC does not believe reports correlated with incidence decline.[11]
2. Measles reports declined as percent of child population. CDC does not believe reports correlated with declining incidence.
3. CDC quoted cases and death ratio "fit" without adjustment. CDC does not believe...
Severe measles infections have been reported in other immunocompromised patients. Measles infection without rash has also been described (7). Physicians caring for patients with HIV infection should be aware that measles can be severe and may occur without the typical rash.
http://www.whale.to/vaccines/mmr.html
Barbara Loe Fisher (NVIC 2006) ...MMR vaccine is known to induce brain inflammation and death within 8 to 14 days after vaccination...
http://www.whale.to/vaccines/immune.html
Vaccines and Immune Suppression citations
Question and Answer from CDC web site: http://www.cdc.gov/vaccines/vpd-vac/combo-vaccines/mmr/faqs-mmr-hcp.htm
Can I give a PPD (tuberculin skin test) on the same day as a dose of MMR vaccine?
A PPD can be applied before or on the same day that MMR vaccine is given. However, if MMR vaccine is given on the previous day or earlier, the PPD should be delayed for at least one month. Live measles vaccine given prior to the application of a PPD can reduce the reactivity of the skin test because of mild suppression of the immune system.
"Dr. H.H. Fudenberg, world-renowned immunologist with hundreds of publications to his credit, made the following comments: “One vaccine decreases cell-mediated immunity by 50%, two vaccines by 70%…all triple vaccines (MMR, DTaP) markedly impair cell-mediated immunity, which predisposes to recurrent viral infections, especially otitis media, as well as yeast and fungi infections.”
http://www.whale.to/a/yurko.html --Harold E. Buttram, MD; Susan Kreider, RN; Alan R. Yurko
Mercola.com/article/vaccines/immune_suppression.htm
Vaccines and Immune Suppression
OCR for page 52
Adverse Events Associated with Childhood Vaccines: Evidence Bearing on Causality (1994) by Institute of Medicine (IOM)
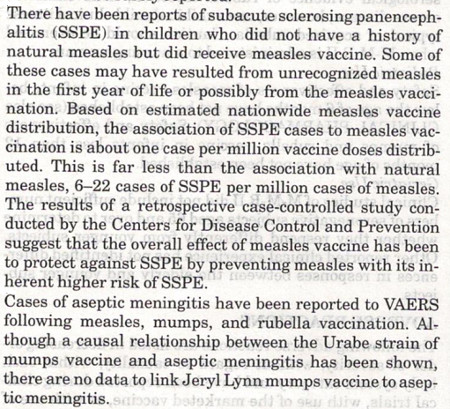
The incidence of SSPE has decreased dramatically since the beginning of immunization with the live attenuated measles virus vaccine (Modlin et al., 1977). Estimates of the incidence of SSPE after natural measles infection range from 5 to 20 cases per 1 million children with clinical measles infection per year (Halsey et al., 1978).
OCR for page 122
The annual incidence of encephalitis for the years 1950 to 1981 in Olmsted County, Minnesota, was 7.4 per 100,000 people (Beghi et al., 1984; Nicolosi et al., 1986).
The incidence in children less than age 1 year was 22.5, in children between ages 1 and 4 years it was 15.2, and in children between ages 5 and 9 years it was 30.2 per 100,000.
Other estimates of encephalopathy for children less than age 2 years were somewhat lower than those reported by Beghi et al. and Nicolosi et al. cited above.
Other estimates for annual incidence range from 5 per 100,000 people (Walker et al., 1988) to 10 per 100,000 people (Gale et al., 1990). Chapter 3 contains a discussion of encephalopathy.
Subacute Sclerosing Panencephalitis and the Salk Vaccine
Lancet 6 Oct. 1973
Summary
From 1956 to 1966 the incidence of subacute sclerosing panencephalitis (s.s.p.e.) in the northern half of the North Island of New Zealand was approximately one hundred times greater than might be expected. No case was seen before 1956, and none has been seen since 1969. The incidence of the disease was greatest in the late 1950's, then it waned and was associated with an increasing age at onset of symptoms. Mass vaccination of primary-school children with Salk vaccine was begun in 1956. The vaccine used is likely to have contained live SV40 virus. Killed measles virus is another possible contaminant. It is believed that the administration of Salk vaccine in New Zealand was related to the appearance of s.s.p.e. in the community. The idea that an unusual reaction to measles infection is the sole cause of s.s.p.e. is not consistent with the observations in new Zealand.
The measles vaccination was first promoted to prevent subacute sclerosing panencephalitis (SSPE), an extremely rare complication of measles. Symptoms of SSPE are identical to autism; repetitive motions, more boys affected than girls, the onset of mental deterioration is the presenting symptom as reported by Harrisons. It continues to say that it may be related to measles vaccination.
The CDC's website suggests that SSPE has been eradicated due to vaccination for measles; yet the 2010 PDR Guide Drug Interactions, side effects and Indications lists under the Heading Panencephalitis, sclerosis, subacute - three drugs that would CAUSE this condition: Attenuvax, M-M-R II and ProQuad. All are Measles Mumps and Rubella vaccinations.
The suggestion by the CDC that SSPE has been eradicated by a substance (vaccine) that causes it is clearly an impossibility. It appears that SSPE has been rebranded Autism. It is a synonym.
Thanks to Susan Maple for this section.
See "More References" below for manufacturer's Package Inserts relative to MMR and SSPE.
Also see section "Are vaccine induced measles cases more or less mild than natural measles cases?" for more on SSPE.
- Package Insert for MMR_II: http://www.merck.com/product/usa/pi_circulars/m/mmr_ii/mmr_ii_pi.pdf
- Sources for information on Vitamins A and C in reducing measles side effects and deaths:
http://www.whale.to/m/measles.html
http://www.vaclib.org/basic/trufax/v4.html
http://www.vaclib.org/intro/present/index2.htm - Seeking An Alternative by Ian Sinclair http://www.vaclib.org/basic/health/alternative.htm
- Adverse Events Associated with Childhood Vaccines: Evidence Bearing on Causality (1994) by Institute of Medicine (IOM)
http://books.nap.edu/openbook.php?record_id=2138&page=118 "Whatever its toll in industrialized countries, where the measles fatality rate is 1 per 10,000 cases (Babbott and Gordon, 1954), measles has been a far greater scourge in developing countries, with case fatality rates as high as 1,000 per 10,000 cases (Morley, 1974)." - DISPELLING VACCINATION MYTHS: by Alan Phillips, VACCINATION MYTH #3:
http://www.vaclib.org/docs/myths.htm - University of Maryland Medical Center: Scroll down to: Side Effects of Live Measles Mumps-Rubella (MMR) Vaccines
http://web.archive.org/web/20070102054223/http://www.umm.edu/patiented/articles/what_vaccines_measles_mumps_rubella_000090_4.htm - Vaccine Safety Manual by Neil Z. Miller, Measles Chapter, following topics:
A higher nutritional status, especially Vitamin A, lowers measles associated death rate.
Use of anti-fever medicines (aspirin, etc) increases measles associated death rate.
In Africa, a study showed more severe disease (higher fever) was associated with HIGHER survival rate.
An increase in Neurological adverse effects followed measles vaccination.
A history of high titer measles vaccination. - Autism and MMR: Something is Rotten in Denmark
http://vaclib.org/basic/mmr-errors.htm - Antibody titers and immunity: Are they related? vaclib.org/basic/titers-immunity.htm
-
Source of CDC History statements.
http://web.archive.org/web/20070204040817/http://www.cdc.gov/nip/diseases/measles/history.htm - Varicella-incidence.pdf http://vaclib.org/legal/MTstate/Varicella-incidence.pdf
Scan of MMR_II from 2007 PDR 2007-PDR-on-MMRII.pdf [6 MB PDF]
Thumbnail of SSPE section 2007MMRiiPI.jpg [107 KB]
Additional Links and references:
[A "live" measles vaccine was introduced in the same year, 1963, as the first measles vaccine, the Killed Measles Virus (KMV).]
http://www.whale.to/vaccines/measles.html
MMR/MR vaccine deaths http://www.whale.to/vaccine/mmr2.html
Data for graphs created above, unless otherwise credited are from Colonial Times to 1970 Census information: CT1970p1-02.pdf and CT1970p1-03.pdf. Census documents may be downloaded here: http://www.census.gov/prod/www/abs/statab.html
Some good questions for the student of natural health principles:
Why did only 90% of children have measles in the first15 years of life?
Why did it take 15 years to reach 90%?
What happened to the 90 % figure in the prevaccine era?
Did the 90% go down without the CDC being aware it it?
Can a reporting system over-report?